January 13, 2026 12 mins
Workforce-Focused Analysis on GLP-1s: Phase Two Findings

Explore second-phase GLP-1 study insights on improved medical cost growth, adherence and women’s health.
Introduction
Aon’s workforce-focused GLP-1 analysis was designed to help employers understand the long-term impact of covering second-generation GLP-1 medications – such as Mounjaro, Ozempic, Wegovy and Zepbound – for diabetes and weight management. Building on Aon’s initial analysis conducted in May 2025, the second phase of research expanded the study to include a larger, nationally representative sample of 192,000 GLP-1 users. To ensure robust comparisons, GLP-1 users were matched to non-users with similar demographic and clinical profiles, to create a control group of "digital twins".
The analysis leveraged de-identified commercial medical and pharmacy claims data from approximately 50 million commercial lives, allowing for a comprehensive evaluation of medical costs, clinical outcomes and adherence patterns over extended timeframes. This study is independent and agnostic to the specific drug, drug maker and insurance carrier or provider. The research is intended to provide employers with an independent longitudinal study to reference when making plan design, benefit and coverage decisions.
Key Findings
Diabetes-related findings: Over a 30-month period, users of GLP-1s for diabetes experienced a slower increase in medical cost growth compared to non-users. The clinical benefits, including reductions to hospitalizations due to MACE continue to be observed in the second analysis.
Weight loss-related findings: Individuals using GLP-1s for 18 months show the same pattern of reduced medical cost growth, reductions in hospitalizations due to MACE and lower claims incidence for a range of conditions.
Adherence: Adherence is a critical driver of value. GLP-1 users who maintain at least 80 percent adherence to therapy see greater cost reductions, and statistically significant decreases in MACE hospitalizations and condition incidence than those with lower adherence.
Women’s health: Female GLP-1 users are more likely to see reductions in hospitalizations for MACE, alcohol abuse, bariatric surgery and pancreatic disorders compared to males. It is notable that a higher proportion of GLP-1 weight loss users are women, and we are observing additional promising impacts on a range of women's health conditions. Women GLP-1 users were observed to have lower incidence of ovarian cancer, breast cancer and osteoporosis than female non-users. Conversely, women GLP-1 users experience higher rates of hospitalization for gallbladder surgery than men.
Improved Medical Spend Growth: Weight Loss and Diabetes Cohort Findings
The second phase of analysis confirms and expands on earlier findings, showing that – following an initial increase – GLP-1 users in both the weight loss and diabetes cohorts experience slower medical cost growth (medical and non-GLP-1 pharmacy spend) compared to non-users.
Individuals using GLP-1s for diabetes experienced a six percentage point improvement in medical spend growth compared to the control group between 12 months and 30 months post GLP-1s initiation. Users with at least 80 percent adherence experienced a nine percentage point improvement compared to the control group.
Users of GLP-1s indicated for weight loss experienced a three percentage point improvement compared to the control group between 12 months and 18 months post GLP-1s initiation. Users with at least 80 percent adherence experienced a seven percentage point improvement compared to the control group.
These results underscore the importance of adherence to GLP-1 drug therapy in observed decreases to cost growth over the study period.
Medical and pharmacy claims cost for users of Mounjaro and Ozempic (treatment group) vs control over 30 months, compared to control group.
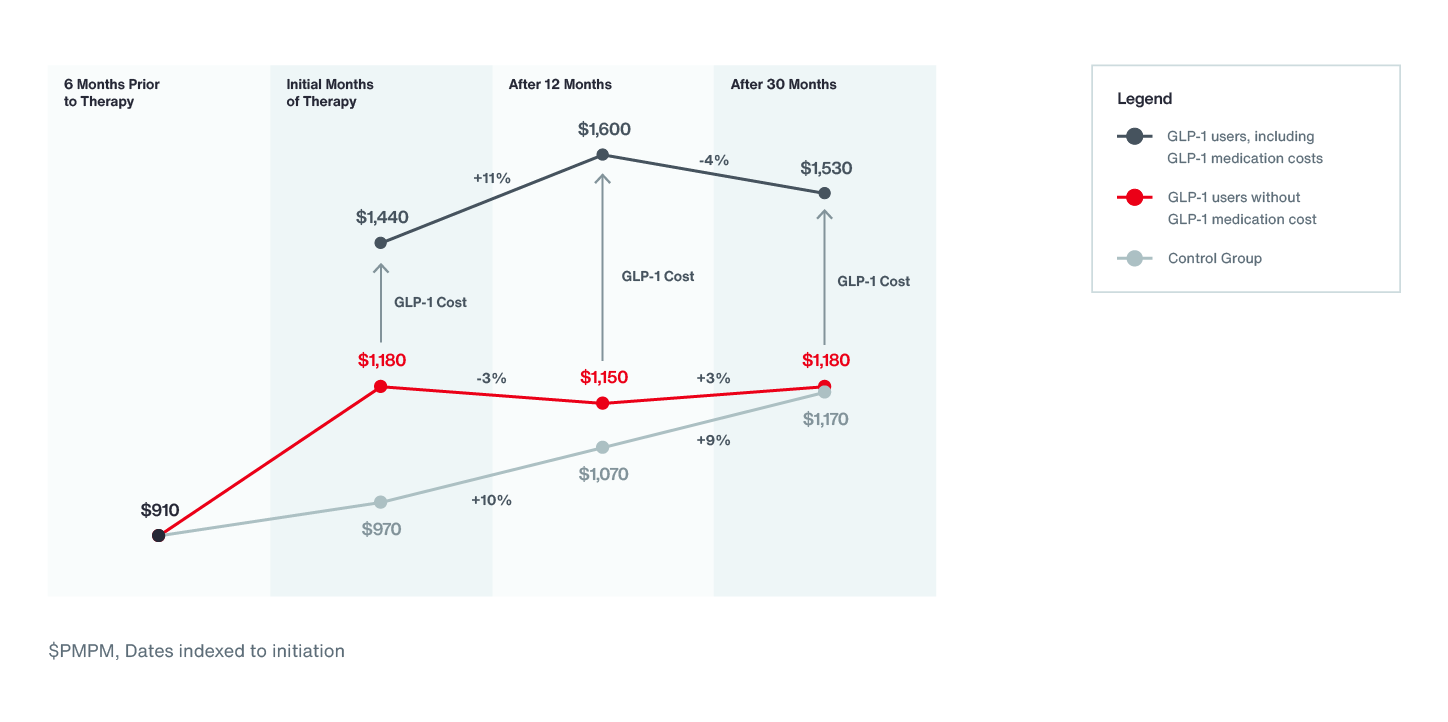
Note: Rounds to nearest $10 and integer trends. Includes claims incurred Nov ’21 – Mar. ’25 (Paid through June ’25). Excludes users with <20% GLP-1 days supplied filed over time for which we can observe the individual. Does not factor in member cost share. Assumes flat 35% rebate on all pharmacy benefit brand medications.
Medical and pharmacy claims cost for users of Wegovy and Zepbound (treatment group) vs control over 18 months, compared to control group.
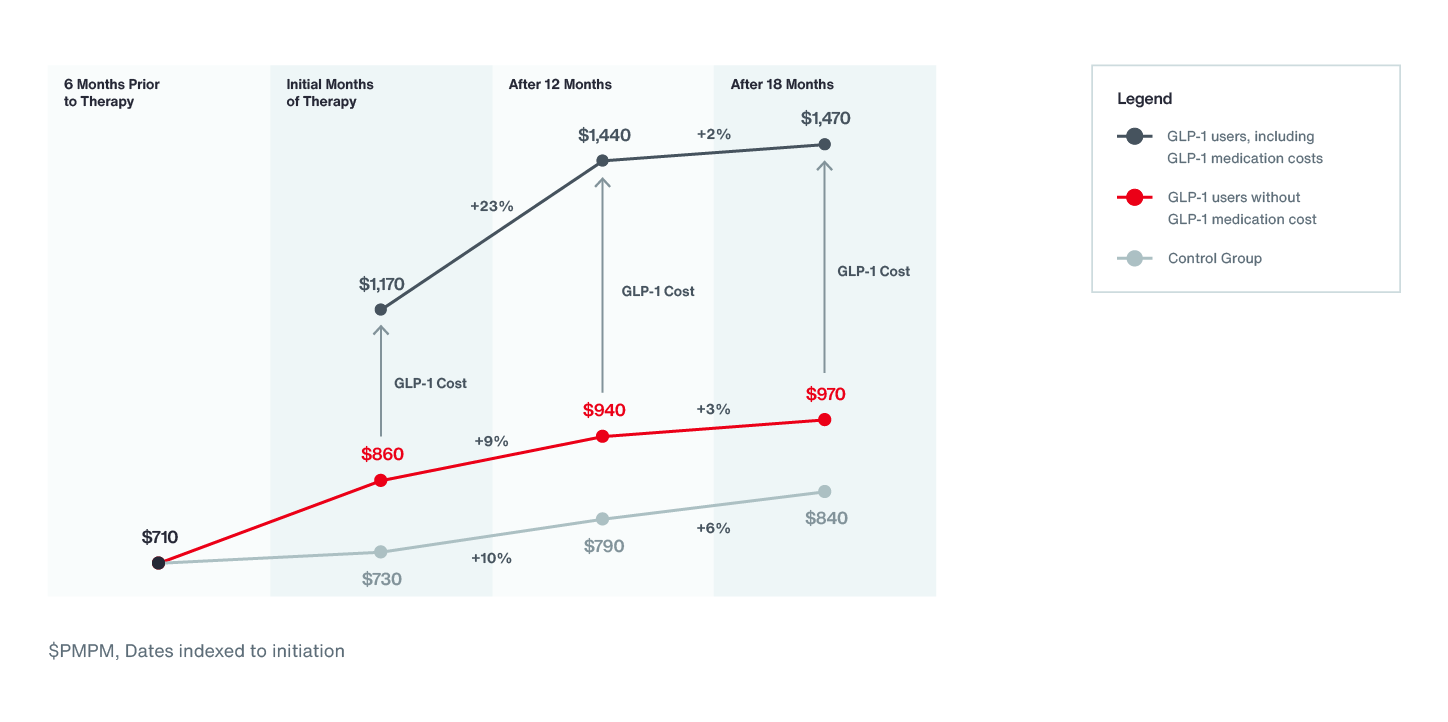
Note: Rounds to nearest $10 and integer trends. Includes claims incurred Nov ’21 – Mar. ’25 (Paid through June ’25). Excludes users with <20% GLP-1 days supplied filed over time for which we can observe the individual. Does not factor in member cost share. Assumes flat 35% rebate on all pharmacy benefit brand medications.
Women’s Health Outcomes
In Aon’s study, GLP‑1 users experienced a 37 percent reduction in hospitalizations caused by MACE (including stroke, heart attack and heart failure) over the 24 months following GLP-1 therapy initiation. Women accounted for 63 percent of GLP-1 users in this study, and among female GLP-1 users Aon observed a 47 percent reduction in hospitalizations for MACE compared to the female control group. This represents a much larger reduction compared to the 26 percent reduction observed in male GLP-1 users compared to the male control group. This observed cardiovascular benefit carries a significant implication for employers, especially in workforce demographics with high cardiometabolic risk.
Beyond cardiovascular health, Aon observed that female GLP-1 users had an approximately 50 percent lower incidence rate for ovarian cancer and 14 percent lower incidence of breast cancer compared to matched female non-users. Furthermore, these women showed a 16 percent reduction in incidence of osteoporosis alongside lower rates of several other chronic conditions such as rheumatoid arthritis. Female GLP-1 users were also less likely to be hospitalized for alcohol or drug abuse, bariatric surgery, and certain pancreatic disorders compared to female non-users, with this reduction being relatively greater than that observed among male users. Conversely, female GLP‑1 users experienced higher rates of hospitalization for gallbladder surgery than male users.
Although claims data cannot establish direct causality, these consistent patterns suggest that GLP-1 therapy may offer health advantages for women, extending beyond weight management, glycemic control and traditional cardiovascular outcomes.
Diagnosis rate impact by condition among female GLP-1 utilizers of Mounjaro, Ozempic, Wegovy, and Zepbound during first 24 months compared to control
| Condition | Diagnosis rate impact | Hazard Ratio |
| Breast Cancer | Reduction | 0.86 |
| Ovarian Cancer | Reduction | 0.50 |
| Rheumatoid arthritis | Reduction | 0.91 |
| Osteoporosis | Reduction | 0.84 |
Note: All comparisons are at a 99% confidence interval
Inpatient admission by condition among female GLP-1 utilizers of Mounjaro, Ozempic, Wegovy, and Zepbound during first 24 months compared to control
| Condition | Inpatient admission impact | Hazard Ratio |
| MACE | Reduction | 0.53 |
| Alcohol or Drug Abuse Without Rehab | Reduction | 0.46 |
| Bariatric Surgery | Reduction | 0.21 |
| Pancreatic Disorders | Reduction | 0.27 |
| Gallbladder Surgery | Increase | 1.81 |
Note: All comparisons are at a 99% confidence interval
The Importance of Adherence
Across both diabetes and weight loss cohorts, adherence to GLP-1 therapy at 80% or higher amplifies cost benefits. The study also observed reductions in hospitalizations for MACE among highly adherent GLP-1 users.
These findings indicate that much of the long-term value from GLP-1 therapy relies on members persisting with therapy with adherence rates above 80% to achieve the underlying clinical benefits. Recognizing the impact of GLP-1 adherence rates helps employers make informed decisions about coverage and support strategies for employees.
Medical and pharmacy claims cost for user of Mounjaro and Ozempic (treatment group) vs control over 30 months at 80% adherence, compared to control group.
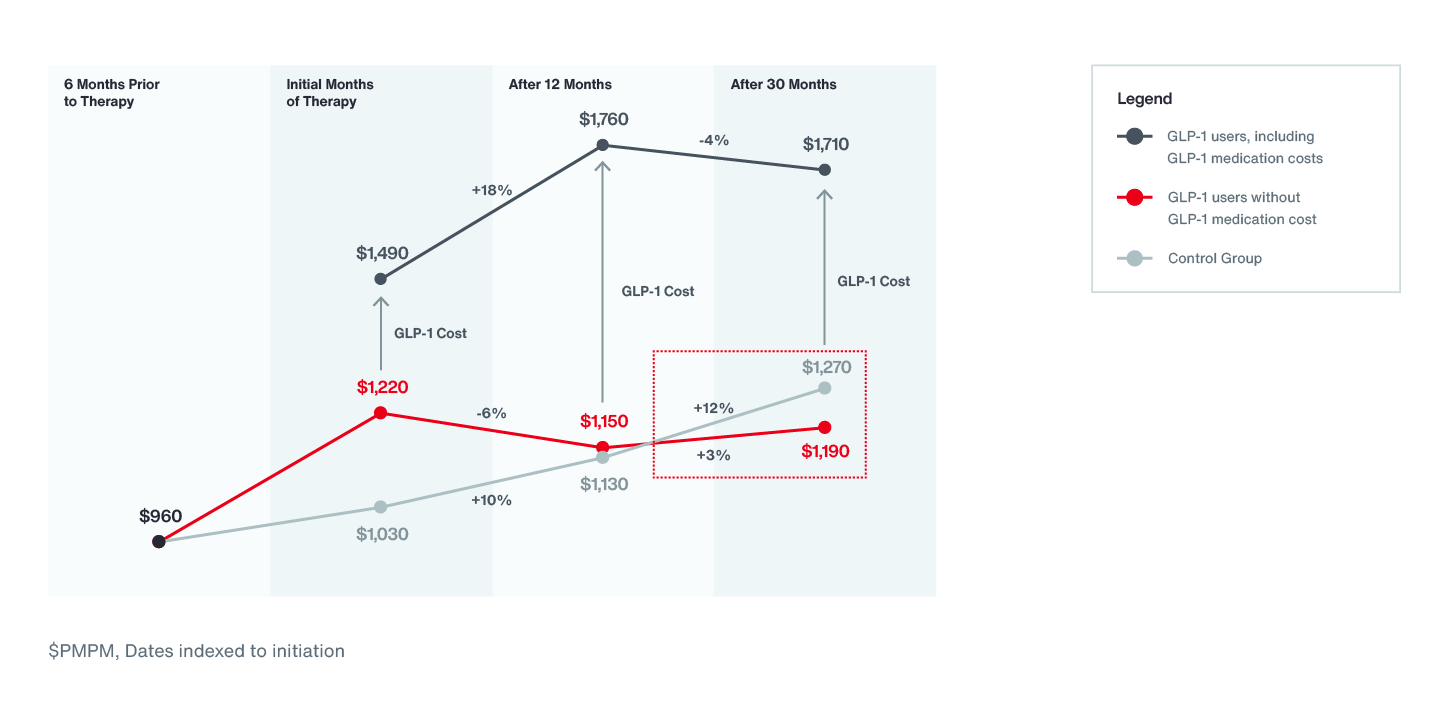
Note: Rounds to nearest $10 and integer trends. Includes claims incurred Nov ’21 – Mar. ’25 (Paid through June ’25). Excludes users with <20% GLP-1 days supplied filed over time for which we can observe the individual. Does not factor in member cost share. Assumes flat 35% rebate on all pharmacy benefit brand medications.
Medical and pharmacy claims cost for user of Wegovy and Zepbound (treatment group) vs control over 18 months at 80% adherence, compared to control group.
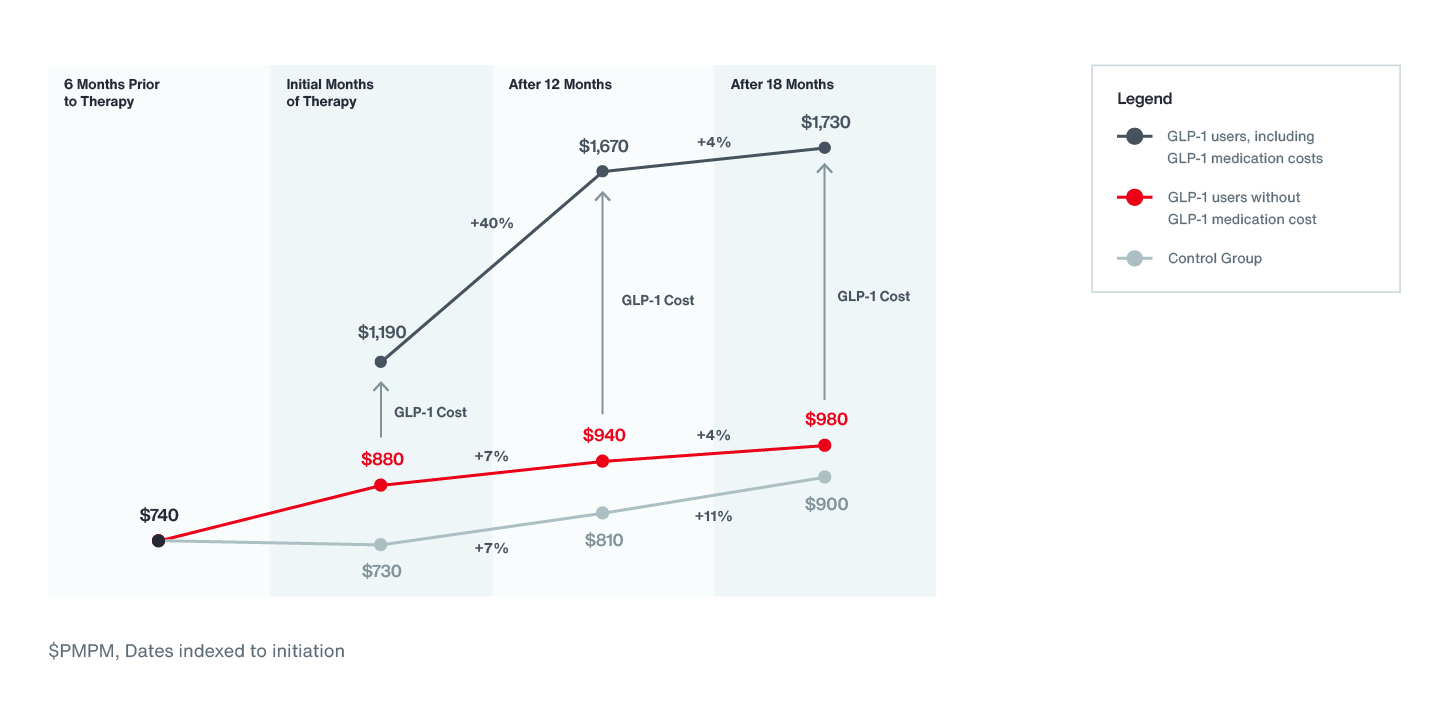
Note: Rounds to nearest $10 and integer trends. Includes claims incurred Nov ’21 – Mar. ’25 (Paid through June ’25). Excludes users with <20% GLP-1 days supplied filed over time for which we can observe the individual. Does not factor in member cost share. Assumes flat 35% rebate on all pharmacy benefit brand medications.
Future Outlook for GLP-1 Costs
Overall costs for GLP-1 users remain higher than those for non-users, largely due to the expense of the medication itself. However, employers are observing favorable medical cost growth reduction for users. Despite these positive shifts, total plan spending continues to exceed that of non-users when drug costs are factored in. It’s important to note that Aon’s analysis is based on retrospective GLP-1 pricing. Looking ahead, the drug pricing will continue to compress with direct-to-consumer programs, innovative pricing models and the approval of oral GLP-1 medications, all likely to influence market dynamics over the next few years.
Considerations for Employers
For employers, these results highlight that decisions about GLP-1 coverage extend beyond short-term drug expenses. Coverage decisions are complex, involving a multitude of factors with applicability that will vary by employer. Recognizing this, our analysis suggests that GLP-1 use with strong adherence is linked with improved employee health outcomes and a slower rise in medical costs over time, even as treatment costs continue to shift. Aon’s 2025 Health Survey saw that two-thirds of respondents are waiting for a higher cost threshold or remain uncertain about when to act. Adherence-related data empowers employers to make informed, nuanced decisions amid evolving pricing models and clinical developments.
Employers should consider that drug prices are likely to compress with expanded direct-to-consumer programs as well as the introduction of newly approved oral formulations, and should weigh clinical benefits and workforce needs among other factors. There is no single approach to plan coverage for all employers but leveraging data and closely monitoring the emerging evidence and market landscape can help employers navigate complex coverage decisions.
Next Steps
Building on these results, Aon is continuing to track GLP-1 utilization, pricing and outcomes as new indications, products and financing models emerge. We are also exploring additional analyses focused on productivity and workforce performance, as well as opportunities to replicate this study among populations in several large countries outside the United States to better understand the global impact of GLP-1 medications.
About Aon’s Workforce Focused GLP-1 Analysis
Study Design and Data Sources
Aon’s GLP-1 analytics are built on deidentified commercial medical and pharmacy claims from multiple national data sets, representing approximately 50 million commercial lives.
Key parameters of the second phase of analysis include:
Study period: GLP-1 initiations between November 2021 and March 2025, with paid claims observed through June 2025.
Population:
- 192,000 GLP-1 users across all indications
- 63 percent female; average age 49 years
Indications:
- 70 percent primarily using GLP-1s for diabetes management
- 30 percent primarily using them for weight loss
- Medications analyzed: Second generation GLP-1s - Mounjaro, Ozempic, Wegovy and Zepbound were included in the analysis.
To ensure robust comparisons, GLP-1 users were matched to non-users with similar demographic and clinical profiles, including age, gender, baseline health care costs, diagnoses and prior use of relevant medications. Individuals without sufficient continuous enrollment, those who filled 90-day or less of a GLP-1, pregnant users and those with specific preexisting conditions were excluded.
Pre‑existing conditions included (1) annual claims exceeding $500,000 in any year 2022–2024 and (2) blood disorders, end stage renal disease, cancer, or prior bariatric surgery during the 6‑month pre‑period before GLP‑1 initiation.
Adherence Measurement
Aon’s analysis uses proportion of days covered (PDC) as the primary adherence metric. In the broader multiyear trend analysis:
- The average PDC among GLP-1 users is approximately 71 percent.
- Half of users maintain over 80 percent adherence.
- For the cumulative incidence and hospitalizations analyses, the study focuses on individuals with more than 80 percent adherence, allowing us to assess the outcomes of near continuous therapy.
PDC is calculated as (number of days covered) / (total days in the time period)
Cohorts and Time Horizons
The second phase of analysis extends and refines the original analysis by separating cohorts by primary indication:
- Diabetes cohort: Individuals with a diabetes indication and GLP-1 use primarily for glycemic control
- Weight loss cohort: Individuals using GLP-1s for obesity or weight management without a diabetes indication
Extending observation periods
- 30-month analysis window for the diabetes cohort
- 18-month analysis window for the weight loss cohort
This approach allows us to evaluate whether the cost and clinical trends seen in the first white paper persist over a longer timeframe and whether they hold consistently across key sub populations.
Aon’s analysis does not reflect:
- The most recent direct-to-consumer pricing options
- Newer strategies such as alternative payment methods, updated pricing agreements or emerging value-based approaches.
- Non-commercially insured groups, such as individuals using compounded formulations, users without insurance or under Medicaid/Medicare.
- Impact of new GLP-1 entrants, including anticipated oral formulations expected to enter the market in 2026, which may materially change price points and member experience.
As a result, the observed relationship between GLP-1 use and total cost in this study should be viewed as a baseline under past pricing conditions, not a forecast of future net cost.
Further reading on GLP-1s and cancer risk:
Glucagon-Like Peptide 1 Receptor Agonists and 13 Obesity-Associated Cancers in Patients With Type 2 Diabetes (JAMA)
GLP-1 Receptor Agonists and Cancer Risk in Adults With Obesity (JAMA)
General Disclaimer
This document is not intended to address any specific situation or to provide legal, regulatory, financial, or other advice. While care has been taken in the production of this document, Aon does not warrant, represent or guarantee the accuracy, adequacy, completeness or fitness for any purpose of the document or any part of it and can accept no liability for any loss incurred in any way by any person who may rely on it. Any recipient shall be responsible for the use to which it puts this document. This document has been compiled using information available to us up to its date of publication and is subject to any qualifications made in the document.
Terms of Use
The contents herein may not be reproduced, reused, reprinted or redistributed without the expressed written consent of Aon, unless otherwise authorized by Aon. To use information contained herein, please write to our team.
Aon's Better Being Podcast
Our Better Being podcast series, hosted by Aon Chief Wellbeing Officer Rachel Fellowes, explores wellbeing strategies and resilience. This season we cover human sustainability, kindness in the workplace, how to measure wellbeing, managing grief and more.
-

Podcast 23 mins
Better Being Series: Understanding Burnout in the Workplace -
Podcast 14 mins
Better Being Series: Why Nutrition Matters -
Podcast 10 mins
Better Being Series: Discover the ‘Blue Zones’ Where People Live Longer -
Podcast 20 mins
Better Being Series: Improving Your Financial Wellbeing -
Podcast 17 mins
Better Being Series: Are You Taking Care of Your Digital Wellbeing? -
Podcast 19 mins
On Aon Podcast: Better Being Series Dives into Women’s Health -
Podcast 25 mins
On Aon’s Better Being Series: Managing Loss and Grief

Aon Insights Series Asia
Expert Views on Today's Risk Capital and Human Capital Issues
-

Article 8 mins
Thriving in an Interconnected World: How the C-Suite Embraces Uncertainty -

Article 6 mins
Powering Progress: Collaborating to Build a Sustainable Future in Emerging Markets -

Article 5 mins
Building Business Resilience: Key Steps to Effectively Integrate Risk Management Across Your Organisation -

Article 7 mins
Why Humans Are the Essential Factor in the Success of Artificial Intelligence (AI) -

Article 5 mins
Leveraging Research and Expertise to Strengthen Your HR Strategy for 2025 and Beyond -
Article 5 mins
Managing Risk on the Energy Transition Journey -

Article 7 mins
The Role of Risk Management in the Age of Generative Artificial Intelligence -

Article 7 mins
Finding A Way In Asia Pacific's New Economic Reality -

Article 4 mins
Three Ways to Boost Value from Benefits: APAC Insights from LinkedIn









Aon Insights Series Pacific
Expert Views on Today's Risk Capital and Human Capital Issues
-

Article 3 mins
Article Template to Duplicate

Aon Insights Series UK
Expert Views on Today's Risk Capital and Human Capital Issues
-

Article 2 mins
Introduction: Clarity and Confidence to Act Now -

Article 11 mins
Navigating a New Age of Macroeconomic Uncertainty -

Article 3 mins
Making Better Decisions — A C-Suite Perspective -

Article 3 mins
Understanding the Dynamics of Today’s Workforce — Reward, Retain, Evolve -

Article 3 mins
Artificial Intelligence — Managing the Risk and Potential -

Article 10 mins
Unlocking Balance Sheet Value to Empower Your Business Strategy -

Article 3 mins
Navigating the Unpredictable: Aon’s Suite of Actionable Analytics -

Article 4 mins
Redefining Risk Capital as a Business Enabler: Veolia's Innovative Approach -

Article 9 mins
A Data-Driven Approach to Better Workforce Decisions -

Article 5 mins
The Importance of Pay Transparency -

Article 6 mins
How Human Capital Data Enhances Risk Management for Financial Institutions -

Article 4 mins
The Battle for Top Talent in the Professional Services Sector -

Article 5 mins
Insights on a Volatile World — Risk Factors That Businesses Need to be Monitoring













Client Trends 2025
Better Decisions Across Interconnected Risk and People Issues.
-

Article 3 mins
Acknowledging Our Complex Reality -

Article 10 mins
Trade in a Technology-Driven Future -

Article 9 mins
How AI and Workforce will Intersect: Navigating Risks and Opportunities -

Article 8 mins
Weather and Workforce: Employers Must Quantify the Risk -

Article 9 mins
Steering Trade and Supply Chains Amid Weather Challenges -

Report 13 mins
Trade Issues Confront Global Businesses on Multiple Fronts -

Report 19 mins
Technology is Driving Firms to Harness Opportunities and Defend Against Threats -

Report 19 mins
Climate Analytics Unlock Capital to Protect People and Property -

Report 14 mins
A Workforce in Transition Prepares to Meet a Host of Challenges









Construction and Infrastructure
The construction industry is under pressure from interconnected risks and notable macroeconomic developments. Learn how your organization can benefit from construction insurance and risk management.
-

Article 8 mins
How North American Construction Contractors Can Mitigate Emerging Risks -

Article 7 mins
Managing Construction Risks: 7 Risk Advisory Steps -
Article 7 mins
Unlocking Capacity and Capital in a Challenging Construction Risk Market -

Article 7 mins
Protecting North American Contractors from Extreme Heat Risks with Parametric -
Article 5 mins
How Climate Modeling Can Mitigate Risks and Improve Resilience in the Construction Industry -

Report 1 mins
Construction Risk Management Europe Report 2023 -

Article 8 mins
Parametric Can Help Mitigate Extreme Heat Risks for Contractors in EMEA





Cyber Resilience
Our Cyber Resilience collection gives you access to Aon’s latest insights on the evolving landscape of cyber threats and risk mitigation measures. Reach out to our experts to discuss how to make the right decisions to strengthen your organization’s cyber resilience.
-

Article 8 mins
Cyber and E&O Market Conditions Remain Favorable Amid Emerging Global Risks -

Article 7 mins
How to Navigate AI-Driven Cyber Risks -

Article 9 mins
Building Resilience in a Buyer-Friendly Cyber and E&O Market -

Article 11 mins
A Middle Market Roadmap for Cyber Resilience -

Article 7 mins
Lessons Learned from the CrowdStrike Outage: 5 Strategies to Build Cyber Resilience -

Article 8 mins
Responding to Cyber Attacks: How Directors and Officers and Cyber Policies Differ -

Article 6 mins
Why Now is the Right Time to Customize Cyber and E&O Contracts







Employee Wellbeing
Our Employee Wellbeing collection gives you access to the latest insights from Aon's human capital team. You can also reach out to the team at any time for assistance with your employee wellbeing needs.
-

Article 8 mins
Employer Strategies for Cancer Prevention and Treatment -

Article 6 mins
The Long-Term Care Conundrum in the United States -

Article 9 mins
Developing a Paid Leave Strategy That Supports Workers and Their Families -

Article 9 mins
4 Ways to Foster a Thriving Workforce Amid Rising Health Costs -

Article 9 mins
The Next Evolution of Wellbeing is About Performance -

Article 6 mins
Three Ways Collective Retirement Plans Support HR Priorities -

Article 9 mins
How the Right Employee Wellbeing Strategy Impacts Microstress and Burnout at Work -
Podcast 13 mins
On Aon Podcast: The Future of Healthcare: Key Factors Impacting Medical Trend Rates -

Article 7 mins
Making Wellbeing Part of a Company’s DNA -

Article 7 mins
A Comprehensive Approach to Financial Wellbeing









Environmental, Social and Governance Insights
Explore Aon's latest environmental social and governance (ESG) insights.
Q4 2023 Global Insurance Market Insights
Our Global Insurance Market Insights highlight insurance market trends across pricing, capacity, underwriting, limits, deductibles and coverages.
-
Article 12 mins
Q4 2023: Global Insurance Market Overview -

Article 13 mins
Top Risk Trends to Watch in 2024


Global Risk Management Survey
Better Decisions Across Interconnected Risk and People Issues.
-

Report 28 mins
A New Era of Converging Risks and Accelerating Disruption -

Article 1 mins
Top 10 Global Risks -

Article 1 mins
Industry Insights: Findings from Aon's Global Risk Management Survey -

Article 1 mins
Regional Results -

Article 41 mins
Country-Level Findings -

Report 5 mins
Methodology and Respondent Demographics






Regional Results
How do the top risks on business leaders’ minds differ by region and how can these risks be mitigated? Explore the regional results to learn more.
-

Article 12 mins
Rethinking Resilience: Addressing Asia Pacific’s Top Risks -

Article 10 mins
Turning Uncertainty into Opportunity: Managing Risk in the EMEA Region -

Article 10 mins
Latin America’s Risk Landscape: Turning Complexity into Competitive Advantage -

Article 10 mins
Rethinking Resilience: Navigating North America’s Evolving Risk Landscape




Impact Report 2025
Explore Aon's corporate sustainability impact and strategy.
-

Article 7 mins
Executive Summary -

Article 13 mins
Aon’s Environmental Sustainability -

Article 15 mins
Supporting Energy Resilience and a Transition to a Low-Carbon Economy -

Article 20 mins
Our Commitment to Our Colleagues -

Article 8 mins
Our Community Impact -

Article 10 mins
Governance -

Article 8 mins
Cyber and Data Security -

Article 11 mins
Redefining Resilience








Top 10 Global Risks
Trade, technology, weather and workforce stability are the central forces in today’s risk landscape.
-

Article 6 mins
Cyber Risk: Turning Uncertainty into Opportunity -

Article 7 mins
Business Interruption: Managing Risk in an Interconnected World -

Article 6 mins
Why Economic Slowdown is an Ongoing Risk for Organizations -

Article 8 mins
Navigating Regulatory and Legislative Change -

Article 5 mins
Increasing Competition Is Intensifying Risk for Organizations -

Article 7 mins
Commodity Price Risk and Material Scarcity: An Escalating and Complex Risk -

Article 9 mins
Supply Chain or Distribution Failure: Navigating the New Normal -

Article 5 mins
Damage to Reputation or Brand: A Critical Risk -

Article 6 mins
Geopolitical Volatility: Preparing for the Unpredictable -

Article 6 mins
Cash Flow and Liquidity Risk: A Rising Challenge










Industry Insights
These industry-specific articles explore the top risks, their underlying drivers and the actions leaders are taking to build resilience.
-

Article 9 mins
Building Resilience to Support Growth in Construction and Real Estate -

Article 10 mins
Managing Risk and Unlocking Opportunity in the Food, Agribusiness and Beverage Industry -

Article 8 mins
Adapting to Disruption: How Financial Institutions are Reframing Risk -

Article 10 mins
Turning Risk into Resilience in the Industrials and Manufacturing Industry -

Article 11 mins
Navigating Risk in Insurance: Turning Complexity into Competitive Advantage -

Article 10 mins
Navigating Risk in Life Sciences: Building Resilience to Support Growth -

Article 11 mins
Navigating Volatility in Natural Resources: Risk Management as a Value Driver -

Article 10 mins
Navigating Risk in Transportation and Logistics: Gearing Up for Big Transitions -

Article 9 mins
Technology, Media and Communications: Rethinking Risk in a Shifting Landscape









Human Capital Analytics
Our Human Capital Analytics collection gives you access to the latest insights from Aon's human capital team. Contact us to learn how Aon’s analytics capabilities helps organizations make better workforce decisions.
-

Article 35 mins
5 Human Resources Trends to Watch in 2025 -
Article 13 mins
Medical Rate Trends and Mitigation Strategies Across the Globe -

Article 9 mins
3 Strategies to Help Avoid Workers Compensation Claims Litigation -
Podcast 15 mins
On Aon Podcast: Using Data and Analytics to Improve Health Outcomes -

Article 14 mins
How Technology Will Transform Employee Benefits in the Next Five Years -
Podcast 18 mins
On Aon Podcast: Technology Impacting the Future of Health and Benefits -

Article 10 mins
Designing Tomorrow: Personalizing EVP, Benefits and Total Rewards




Human Capital Quarterly Insights Briefs
Read our collection of human capital articles that explore in depth hot topics for HR and risk professionals, including using data and analytics to measure total rewards programs, how HR and finance can better partner and the impact AI will have on the workforce.
-

Article 12 mins
Total Rewards Strategies That Drive Business Outcomes -
Article 35 mins
5 Human Resources Trends to Watch in 2025 -

Article 20 mins
5 Ways HR Can Partner with Finance to Drive Growth -

Article 15 mins
How Artificial Intelligence is Transforming Human Resources and the Workforce -

Article 15 mins
Five Big Human Resources Trends to Watch in 2024 -
Article 10 mins
Designing Tomorrow: Personalizing EVP, Benefits and Total Rewards -

Article 10 mins
How Data and Analytics Can Optimize HR Programs -

Article 15 mins
Get Ready for the Top 5 HR Trends in 2023






Insights for HR
Explore our hand-picked insights for human resources professionals.
-

Article 7 mins
COVID-19 has Permanently Changed the Way We Think About Wellbeing -
Article 10 mins
How Data and Analytics Can Optimize HR Programs -

Article 7 mins
Case Study: The LPGA Unlocks Talent Potential with Data -

Article 10 mins
Navigating the New EU Directive on Pay Transparency -

Article 6 mins
Rethinking Your Total Rewards Programs During Mergers and Acquisitions




Workforce
Our Workforce Collection provides access to the latest insights from Aon’s Human Capital team on topics ranging from health and benefits, retirement and talent practices. You can reach out to our team at any time to learn how we can help address emerging workforce challenges.
-
Article 8 mins
Weather and Workforce: Employers Must Quantify the Risk -
Article 12 mins
Total Rewards Strategies That Drive Business Outcomes -

Article 8 mins
AI and Workforce Skills: Who Should Act and Why Now? -

Article 19 mins
3 Strategies to Promote an Inclusive Environment and Bridge the Gender Gap -
Article 8 mins
2025 Salary Increase Planning Tips -
Article 12 mins
People Risks Are Rising: Here’s How U.S. Benefits Are Stepping Up -
Article 8 mins
Employer Strategies for Cancer Prevention and Treatment -

Article 6 mins
Taking a Data-Led Approach to Job Architecture to Accelerate Pay Transparency -
Podcast 12 mins
Better Being Series: Building Sustainable Performance in a Multi-Generational Workforce -

Article 7 mins
Key Trends in U.S. Benefits for 2025 and Beyond -

Article 7 mins
Why Pay Transparency Demands a Total Rewards Lens -
Article 9 mins
4 Ways to Foster a Thriving Workforce Amid Rising Health Costs





Mergers and Acquisitions
Our Mergers and Acquisitions (M&A) collection gives you access to the latest insights from Aon's thought leaders to help dealmakers make better decisions. Explore our latest insights and reach out to the team at any time for assistance with transaction challenges and opportunities.
-
Article 6 mins
Rethinking Your Total Rewards Programs During Mergers and Acquisitions -

Article 9 mins
Organizational Design and Talent Planning are Key to M&A Success -

Article 5 mins
Project Management for HR: The Secret Behind a Successful M&A Deal -

Article 8 mins
Cultural Alignment Planning Drives M&A Success -

Report 1 mins
A Guide to Maximizing Value in Post-Merger Integrations -

Report 2 mins
The ABC's of Private Equity M&A: Deal Flow Impacts of Al, Big Tech and Climate Change -
Article 11 mins
The Silver Lining on M&A Deal Clouds: M&A Insurance Insights from 2023





Natural Resources and Energy Transition
The challenges in adopting renewable energy are changing with technological advancements, increasing market competition and numerous financial support mechanisms. Learn how your organization can benefit from our renewables solutions.
-

Article 4 mins
5 Steps for Successful Carbon Accounting Verification -

Article 6 mins
AI Innovations in Renewable Energy: Transforming the Sector -

Article 11 mins
Securing Human Capital in Natural Resources -

Article 6 mins
Decarbonizing Construction for a Low-Emission Future




Navigating Volatility
How do businesses navigate their way through new forms of volatility and make decisions that protect and grow their organizations?
Parametric Insurance
Our Parametric Insurance Collection provides ways your organization can benefit from this simple, straightforward and fast-paying risk transfer solution. Reach out to learn how we can help you make better decisions to manage your catastrophe exposures and near-term volatility.
-

Article 10 mins
How Public Entities and Businesses Can Use Parametric for Emergency Funding -

Article 6 mins
Parametric Insurance: A Complement to Traditional Property Coverage -

Article 8 mins
Using Parametric Insurance to Match Capital to Climate Risk -

Article 6 mins
Using Parametric Insurance to Close the Earthquake Protection Gap -
Article 5 mins
How Technology Enhancements are Boosting Parametric




Pay Transparency and Equity
Our Pay Transparency and Equity collection gives you access to the latest insights from Aon's human capital team on topics ranging from pay equity to diversity, equity and inclusion. Contact us to learn how we can help your organization address these issues.
-
Article 6 mins
Taking a Data-Led Approach to Job Architecture to Accelerate Pay Transparency -
Article 19 mins
3 Strategies to Promote an Inclusive Environment and Bridge the Gender Gap -

Report 1 mins
The 2024 North America Pay Transparency Readiness Study -

Article 10 mins
How Financial Institutions can Prepare for Pay Transparency Legislation -

Article 8 mins
Pay Transparency Can Lead to Better Equity Across Benefits -

Article 12 mins
Understanding and Preparing for the Rise in Pay Transparency -
Podcast 14 mins
On Aon Podcast: Understanding Pay Transparency Regulations -
Article 10 mins
Navigating the New EU Directive on Pay Transparency -

Article 6 mins
To Disclose Pay or Not? How Companies are Approaching the Pay Transparency Movement -
Podcast 19 mins
On Aon Podcast: Better Being Series Dives into Women’s Health -

Article 11 mins
Advancing Women’s Health and Equity Through Benefits and Support






Property Risk Management
Forecasters are predicting an extremely active 2024 Atlantic hurricane season. Take measures to build resilience to mitigate risk for hurricane-prone properties.
-
Article 8 mins
Florida Hurricanes Not Expected to Adversely Affect Property Market -

Article 10 mins
Build Resilience for an Extremely Active Atlantic Hurricane Season -

Article 4 mins
Four Steps to Develop Strong Property Risk Coverage in a Hardening Market -
Podcast 16 mins
On Aon Podcast: Navigating and Preparing for Catastrophes -
Article 6 mins
Parametric Insurance: A Complement to Traditional Property Coverage -

Article 4 mins
Navigating Climate Risk Using Multiple Models and Data Sets -

Article 5 mins
Rising Losses From Severe Convection Storms Mostly Explained by Exposure Growth -
Article 6 mins
Using Parametric Insurance to Close the Earthquake Protection Gap




Technology
Our Technology Collection provides access to the latest insights from Aon's thought leaders on navigating the evolving risks and opportunities of technology. Reach out to the team to learn how we can help you use technology to make better decisions for the future.
-
Article 9 mins
How AI and Workforce will Intersect: Navigating Risks and Opportunities -

Article 23 mins
The AI Data Center Boom: Strategies for Sustainable Growth and Risk Management -
Article 8 mins
AI and Workforce Skills: Who Should Act and Why Now? -
Article 7 mins
How Technology is Transforming Open Enrollment in the U.S. -

Article 15 mins
Navigating Cyber Risks in EMEA: Key Insights for 2025 -
Article 7 mins
How to Navigate AI-Driven Cyber Risks -
Article 15 mins
How Artificial Intelligence is Transforming Human Resources and the Workforce -
Podcast 9 mins
On Aon Podcast: How has CrowdStrike Changed the Cyber Market? -

Article 18 mins
5 Ways Artificial Intelligence can Boost Claims Management -

Article 12 mins
Navigating AI-Related Risks: A Guide for Directors and Officers -
Article 5 mins
How Technology Enhancements are Boosting Parametric -

Article 7 mins
How to Futureproof Data and Analytics Capabilities for Reinsurers





Trade
Our Trade Collection gives you access to the latest insights from Aon's thought leaders on navigating the evolving risks and opportunities for international business. Reach out to our team to understand how to make better decisions around macro trends and why they matter to businesses.
-
Article 10 mins
Trade in a Technology-Driven Future -
Podcast 9 mins
Special Edition: Global Trade and its Impact on Supply Chain -

Article 8 mins
The Evolving Threat of Cargo Theft: 5 Key Mitigation Strategies -
Report 1 mins
Findings from Aon's Global Risk Management Survey | Tenth Edition -
Article 4 mins
Four Steps to Develop Strong Property Risk Coverage in a Hardening Market -

Article 14 mins
Cutting Supply Chains: How to Achieve More Reward with Less Risk -

Article 9 mins
Driving Private Equity Value Creation Through Credit Solutions -
Article 7 mins
4 Steps to Help Take Advantage of a Buyer-Friendly Directors' & Officers' Market -
Article 8 mins
Managing Reputational Risks in Global Supply Chains -

Article 8 mins
How an Outsourced Chief Investment Officer Can Help Improve Governance and Manage Complexity -

Article 8 mins
Decarbonizing Your Business: Finding the Right Insurance and Strategy -

Article 8 mins
Reputation Analytics as a Leading Indicator of ESG Risk






Transaction Solutions Global Claims Study
Better Decisions Across Interconnected Risk and People Issues.
-

Report 5 mins
Chapter 1: Author’s Note & Executive Summary -

Report 8 mins
Chapter 2: North America: Highlights, Claims Severity and Frequency -

Report 3 mins
Chapter 3: North America: Breach Type and Notification -

Report 24 mins
Chapter 4: North America: Industry Sectors and Trends -

Report 5 mins
Chapter 5: North America: Tax Insurance Claims -

Report 5 mins
Chapter 6: EMEA: Highlights and Introduction -

Report 9 mins
Chapter 7: EMEA: Claim Frequency and Metrics -
Report 7 mins
Chapter 8: EMEA: Notifications by Target Location and Claims Severity and Payment Trends -

Report 10 mins
Chapter 9: EMEA: Breach Types and Trends -

Report 7 mins
Chapter 10: EMEA: Case Law, Insurer Survey, Claims Handling and Tax -

Report 6 mins
Chapter 11: APAC: Asia -

Report 9 mins
Chapter 12: APAC: Pacific











Weather
With a changing climate, organizations in all sectors will need to protect their people and physical assets, reduce their carbon footprint, and invest in new solutions to thrive. Our Weather Collection provides you with critical insights to be prepared.
-
Article 9 mins
Steering Trade and Supply Chains Amid Weather Challenges -
Podcast 9 mins
On Aon Podcast: Climate Impact on the Property and Casualty Market -

Alert 14 mins
L.A. Wildfires Highlight Urgent Need for Employee Support and Business Resilience -

Report 3 mins
2026 Climate and Catastrophe Insight -
Article 10 mins
How Public Entities and Businesses Can Use Parametric for Emergency Funding -
Podcast 12 mins
On Aon Podcast: Tackling Climate Risk to Build Economic Resilience -

Article 5 mins
Understanding Freeze Risk in a Changing Climate -
Podcast 9 mins
On Aon Podcast: Climate Science Through Academic Collaboration -
Article 6 mins
How Companies Are Using Climate Modeling to Improve Risk Decisions -
Article 8 mins
Using Parametric Insurance to Match Capital to Climate Risk -

Article 9 mins
Record Heatwaves: Protecting Employee Health and Safety




Workforce Resilience
Our Workforce Resilience collection gives you access to the latest insights from Aon's Human Capital team. You can reach out to the team at any time for questions about how we can assess gaps and help build a more resilience workforce.

More Like This
-

Article 16 mins
People, Power and Water are Defining Digital Infrastructure Operational Risks
As data centers scale into critical infrastructure, the constraints determining success are changing. Power, water and workforce availability are strategic design decisions that shape bankability, insurability and resilience long before a facility becomes operational.
-

Article 9 mins
Insurers’ Opportunities in M&A: The Rise of Hybrid Growth Pathways
As insurance consolidation becomes more selective, insurers are looking beyond full acquisition as the default route to growth. Hybrid pathways may provide capital-efficient access to capabilities and talent, while requiring careful management of governance, execution and alignment risks.
-

Article 17 mins
Insurers’ Opportunities in M&A: When Buying Fits, When Building Wins
Insurers’ growth decisions are entering a more complex phase. As markets soften, capital costs rise and structured volatility pressures balance sheets, insurers are reassessing when consolidation creates real value — and when organic or alternative strategies may deliver better outcomes.



